


Right to Work laws, in effect in 28 states, provide that no person can be compelled, as a condition of employment, to join or not to join, nor to pay dues to a labor union. The right of states to enact such laws is affirmed in §14(b) of the Taft Hartley Act (https://tinyurl.com/y7vewhfj). However, more than 25% of American workers have no right to work at their chosen occupation without a government-approved license, a proportion that has increased five-fold since the 1950s, writes Laurence Vance (https://tinyurl.com/yapyvjf2).
“A license is what you get when the government steals your rights and sells some of them back,” stated Linda Gray Murphy of the American Board of Physician Specialties (ABPS) at our 74th annual meeting. Consumer protection against incompetent or unethical practitioners is always the rationale, although the idea is generally proposed by practitioners, not the public, and the result is always to raise fees and shut out competition.
Licensure boards are politically appointed and have extensive sovereign immunity. Physicians have very few rights, and courts are reluctant to overturn decisions of supposed experts. AAPS legislative efforts to strip the Texas Medical Board of key powers met with some limited success. For example, the board is now required to accept the findings of fact and law by the administrative law judge (ALJ), the change most strenuously resisted by the medical board’s defenders (jpands.org/vol16no3/schlafly.pdf).
Physicians who have served on medical boards report that actions often appear arbitrary. Dangerous doctors escape unscathed despite patient complaints; others are pursued relentlessly on questionable pretexts, even if patient outcomes are exemplary. Two such doctors spoke at our 74th annual meeting in Tucson.
A pioneer in off-pump coronary artery surgery, who taught the technique to many, Dwight Lundell, M.D., lost his Arizona medical license (https://tinyurl.com/ycpzj77f) as a consequence of sham peer review apparently instigated by less skillful competitors.
Robert van Boven, M.D., had a “temporary” restriction placed on his license by the Texas Medical Board that has destroyed his ability to practice for more than 2 years. After he had raised multiple concerns about patient safety at Lakeway Regional Medical Center, allegations were made—despite a never-yet-enforced Texas law, HSC §161.134(a), intended to protect whistleblowers against retaliation—of “disruptive behavior” at LRMC and “inappropriate” actions in the treatment of several patients. An extensive review by Administrative Law Judge Hunter Burkhalter concluded that TMB staff had failed to establish the truth of the allegations by a preponderance of evidence. Over the recommendation of staff attorney Chris Palazola, who said that the case had been “wrongly decided” by the ALJ, TMB accepted the ALJ’s Findings of Fact and Conclusions of Law and lifted the restrictions on Dr. Van Boven’s license. As yet, TMB has not withdrawn the Adverse Action Report in the National Practitioner Data Bank, which will continue to cripple his practice.
Dr. Van Boven has filed a lawsuit against the TMB for due process violations and surrogate retaliation. His legal defense fund is https://www.gofundme.com/patient-physician-advocacy-fund.
He hopes that this case can “help facilitate accountability in state licensing agencies…and safeguard the duty of physicians to advocate for patients.” Physicians are afraid to speak out.
“Hospitals are now at odds with their mission,” he stated at our meeting (https://tinyurl.com/yarvsh5h).
Private “Protection” Entities
Medical licensure was initially intended to ensure a minimal level of training and competence, but as doctors began to narrow their scope of practice, specialty societies arose to set standards. The first, the American Board for Ophthalmic Examinations, was chartered in 1917. The National Board of Medical Examiners formed a “Committee on Specialists” in 1932, which became ABMS in 1970 (https://tinyurl.com/y83mj6ve).
Boards soon began issuing time-limited certificates (AAPS News, May 2014). While ABMS hasn’t been able to prove that board-certified and recertified physicians take better care of patients, they do (a) tend to follow national guidelines better and (b) suffer professional discipline less often, likely because of (a). Efforts to make MOC® a requirement for licensure have failed—so far—but private entities such as hospitals and third-party payers are requiring it for medical staff privileges or payment. Thus, supposedly independent professionals need permission to work from both government and its approved “private” allies.
The motive? Some may want to force doctors to practice a certain way, either for commercial gain or out of ideological zealotry. Doctors need to study board-approved protocols constantly; moreover, new “modules” monitor their patient management. But many in the new certification cottage industry care most about getting their lavish salaries and pension plans funded by physicians’ fees, as forensic accountant Charles Kroll detailed in his talk on “Winning the War against MOC and the ABMS Billion Dollar Swamp Creature” (https://tinyurl.com/ybz68rp8).
ABMS has heard physicians’ protests: “It’s official: MOC® Is Dead. Let the Cover-up Begin,” writes Westby Fisher, M.D. (“Dr. Wes”). Already, a new “vision initiative” has been launched by the original MOC® creators (https://tinyurl.com/ydfev53m).
Do physicians have a right to practice their vocation—or a mere privilege granted by an unaccountable public-private partnership?
Physicians Speak on MOC®
- According to a cross-specialty national survey, only 24% of physicians think MOC® activities are relevant to their patients, only 15% feel they are worthy the effort, only 12% think they are well-integrated into their routine, and 81% believe they are a burden. Only 9% think their patients care about their MOC® status (Mayo Clin Proc 2016;91:1336-1345; https://tinyurl.com/y6u8b8go).
- From “Dr. Wes’s” inbox: MOC® is made compulsory through collusive actions of twin paragons of virtue, insurers and hospital corporations. The implied subtext of the “no more high-stakes exams” promise is that the obligatory ABMS MOC® parasite will remain Ebola-like, in some mutated and quiescent form. The AMA’s answer is to place physician puppets in position of power at the ABMS to assure its lucrative international medical data mining project grows ever stronger. State medical societies’ meeting with ABMS was a Jersey boardwalk puppet show populated by unrepresentative and self-aggrandizing narcissists lobbying each other (https://tinyurl.com/yct47r7h).
- The American Board of Psychiatry and Neurology (ABPN) is launching pilot MOC® options and talking about scrapping the written exam (https://tinyurl.com/ydgv2q78). It must have gotten more severe flak from diplomates than it ever expected. “After the revelation that MOC® is nothing more than a non-evidence-based money-making scam, many boards have shifted gears and are now asking, ‘OK, doctors have figured it out; what do we do now?’,” writes Lawrence Huntoon, M.D., Ph.D.
- The American Academy of Neurology’s “victory” in eliminating the Part IV module of MOC, Improvement in Practice (PIP), was short-lived. It’s back, but with more “flexible” options.
- There are hundreds of heartbreaking stories. Parents of children with cancer are denied waivers while their children are undergoing treatment. Physicians on chemotherapy and immunosuppressed are denied waivers to delay testing in public facilities, losing their certification and their jobs. Physicians, feeling isolated and embarrassed after failing their re-certification, are falling into depression and suicide. MOC is a toxic stress that is literally killing doctors. The boards’ unflagging defense of MOC® is immoral (Meg Edison, M.D., https://tinyurl.com/yd4aukfb).
Oregon Health Authority (OHA) Audit
On Nov 29, 2017, Oregon secretary of state Dennis Richardson released the long-awaited OHA audit. Auditors estimated that $88 million was misspent between March 1 and August 31 of 2017 alone. The audit was difficult to complete because under its previous leadership, OHA’s delays, obfuscations, and failure to cooperate with the audit team were so blatant that national standards required disclosure of such lack of cooperation. Auditors concluded: “The amount of wasteful and incompetent spending at OHA has been staggering and has gone on for at least the past four years” (https://tinyurl.com/ya7t86gr).
“The moment the idea is admitted into society that property is not as sacred as the laws of God, and that there is not a force of law and public justice to protect it, anarchy and tyranny commence. If ‘Thou shalt not covet,’ and ‘Thou shalt not steal’ were not commandments of Heaven, they must be made inviolable precepts in every society before it can be civilized or made free.
John Adams, 1787, https://tinyurl.com/3yua9v
ACTION OF THE MONTH
Help spread the message of freedom to young physicians. Give tax-deductible donations to the AAPS Educational Foundation at aapsonline.org/scholarships.
Wanted: Memorabilia for the 75th Annual Meeting
If you have old photographs, correspondence, news clippings, or other items from AAPS history that you are willing to contribute for our history display, please send them to 1601 N. Tucson Blvd., Suite 9, Tucson, AZ 85716.
Voluntary Certification
Government licensure is not the only way to protect patients against unscrupulous or incompetent practitioners. The late Donald Quinlan, M.D., AAPS president in 1974, trained under the British National Health Service. At that time, there was private certification, which was required only to call one’s self “doctor.”
Vance (op.cit.) argues that licensure is not a proper function of government, and that private certification works well. The National Institute for Automotive Service Excellence (ASE) is his example. Non-ASE certified mechanics may work; repair shops and customers make the choice.
The Ethical Problem with Choice
Of five values to guide health system reform—universal access, equitable access, affordable access, quality, and choice—the last is “the one value that is deeply flawed,” writes Lawrence O. Gostin, J.D. “There is little evidence that individuals can [choose] accurately. But, if they could, it would widen inequalities, because the better-educated and more affluent would likely make more informed choices—leaving the poor and less-educated behind…. There are marked asymmetries in information and market power” (JAMA 12/12/17, https://tinyurl.com/ycfsdzd4).
Using Math without a License
Mat Järlström, an electronics engineer trained in Sweden, challenged a 1959 formula for calculating traffic light length, and shared his findings publicly. After investigating him for 2 years, the Oregon State Board of Examiners for Engineering and Land Surveying fined him $500 for practicing engineering without a license (https://tinyurl.com/ybc5nlq5). In a court case in which Järlström was represented by the Institute for Justice, the Board finally admitted that it had overstepped its authority and refunded the fine (https://tinyurl.com/yczgxpgg), but is trying to preserve its authority to restrict who can talk about or critique engineering principles. About 2 million people practice engineering in the U.S., but only 481,717 were licensed in 2016 (https://tinyurl.com/ksotyk5).
AAPS Calendar
Jan 27. Florida chapter meeting and golf scramble, Tampa, FL.
Apr 6. Thrive Not Just Survive and board meeting, Atlanta, GA.
Oct. 3-6. 75th annual meeting, Indianapolis, IN.
AAPS Has Leave to Amend ABMS Anti-Trust Suit
The federal court in the Northern District of Illinois has granted leave to AAPS to provide more detail as to how Maintenance of Certification (MOC®) harms patients in AAPS v. American Board of Medical Specialties, 14-cv-2705-ARW (N.D. Ill. Dec. 13, 2017). Because antitrust laws exist to protect consumers, not competitors, the court is requiring further specificity as to the harm to patients that is allegedly inflicted by MOC®.
In addition, the court wonders whether the American Board of Medical Specialties (ABMS) and other MOC-related organizations have any control over insurance companies to require MOC® as a condition of participating in their plans. To the extent anyone is aware of a specific relationship between ABMS and insurance companies, or a mechanism by which ABMS may have some influence with insurers, then please let AAPS know.
AAPS plans to add to its allegations ways in which representations made by ABMS and board-certifying societies harm physicians who decline to participate in MOC®. In the past some board-certifying societies have posted disparaging statements about physicians who do not waste the substantial time and money on remaining current with onerous MOC® requirements. For now, the court considers some of these pro-MOC® statements to be mere opinion, which is not actionable, but AAPS can submit stronger examples of unfair disparagement with its upcoming amended complaint.
This legal struggle is far from over, and AAPS observes that earlier this year a district court in New Jersey held there is a valid claim for an antitrust violation by how membership in the American Osteopathic Association is required as a condition of maintaining certification by D.O.s.
The AAPS case was initially filed in New Jersey in 2013 (https://tinyurl.com/ycndp3rx), and the courts have not acted until now, except to grant an ABMS motion to change the venue to Chicago. In dismissing the case as pled, the Court focused on the “voluntary” nature of MOC®. It had not been demonstrated that ABMS has sufficient market power to restrain trade, decrease output, or raise prices. “Antitrust laws protect competition, not competitors” (https://tinyurl.com/yapc4no5). Patients can supposedly find another doctor, or another hospital—somewhere.
FDA Blocks Mosquito Control
In 2009, the U.S. Food and Drug Administration seized control of genetically engineered animals, claiming that “intentionally altered genomic DNA” that is in a genetically engineered animal “and is intended to affect the animal’s structure or function meets the definition of an animal drug.” Then FDA took 5 years (2011-2016) to approve a few small field trials of a genetically engineered mosquito that requires a certain nutritional supplement. In other countries, it has reduced the population of Aedes aegypti by 90%. FDA faced the regulatory conundrum of proving that a “drug” designed to cause a male mosquito to self-destruct after producing defective, doomed offspring is safe and effective—for the mosquito. Under pressure, FDA ceded regulatory control to the Environmental Protection Agency in January 2017. “This is an exemplar of the sort of regulatory overreach and dysfunction that the Trump administration claims it wants to address,” writes Henry Miller (http://tinyurl.com/yc652lz7).
!Tip of the Month: If facing an inspection by the Occupational Health and Safety Administration (OSHA), be polite but firm. Assign a point person to take care of communication, and to escort the inspector at all times. Ask to see the inspector’s credentials and the complaint; attach a copy to your notes. Failure to provide details of the complaint, except for the name of the employee who filed it, may be grounds for an appeal. You can demand to see a subpoena or inspection warrant before allowing the inspection to begin. Object if the inspector tries to broaden the scope. Take a photo of the alleged hazard, and of anything the inspector photographs, and ask the reason for his photo. Make a complete record of the visit, and ask about the process. You may wish to obtain help from your attorney (Medical Practice Compliance Alert, November 2017). If available, you might have an assistant take a video of the visit with your smart phone.
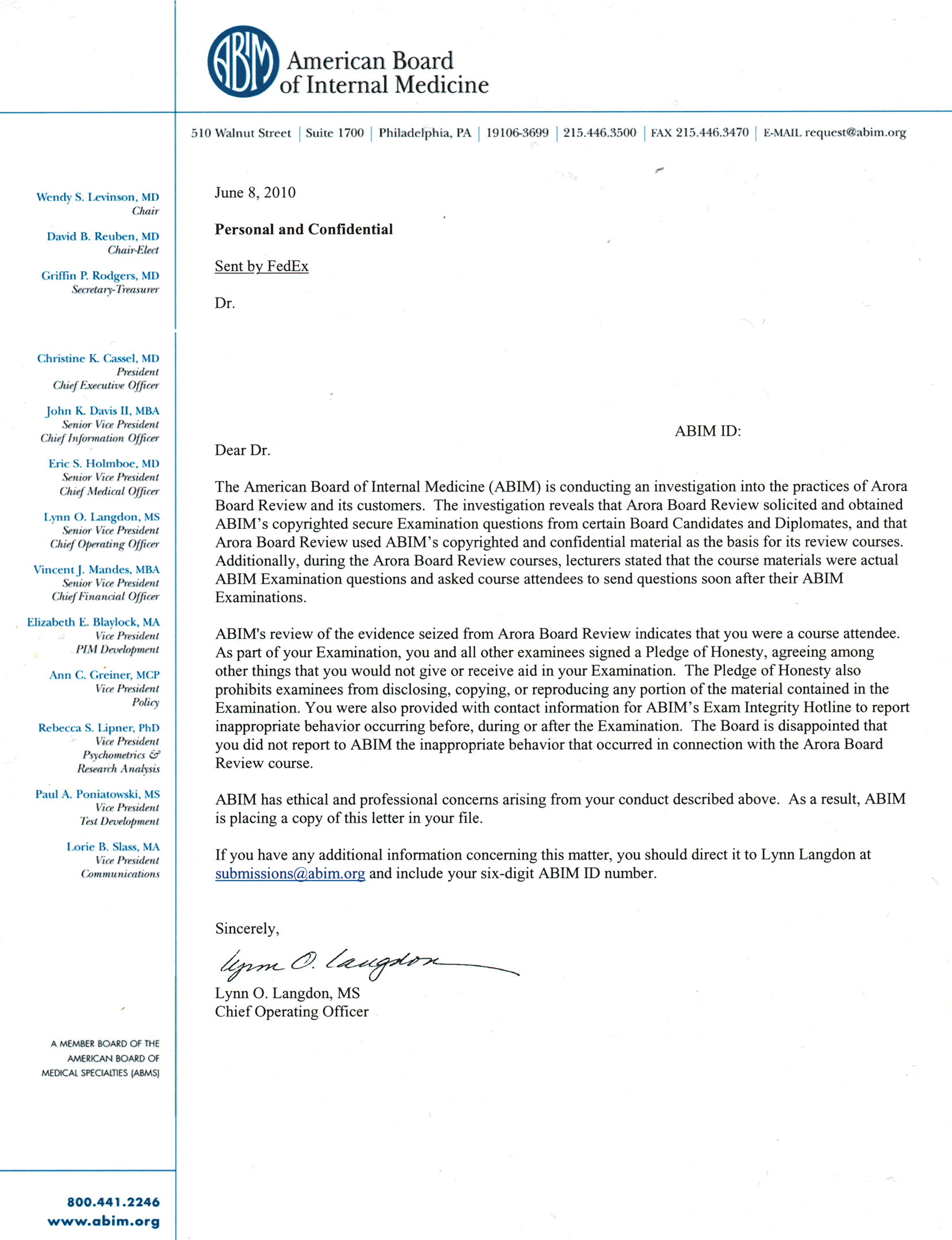
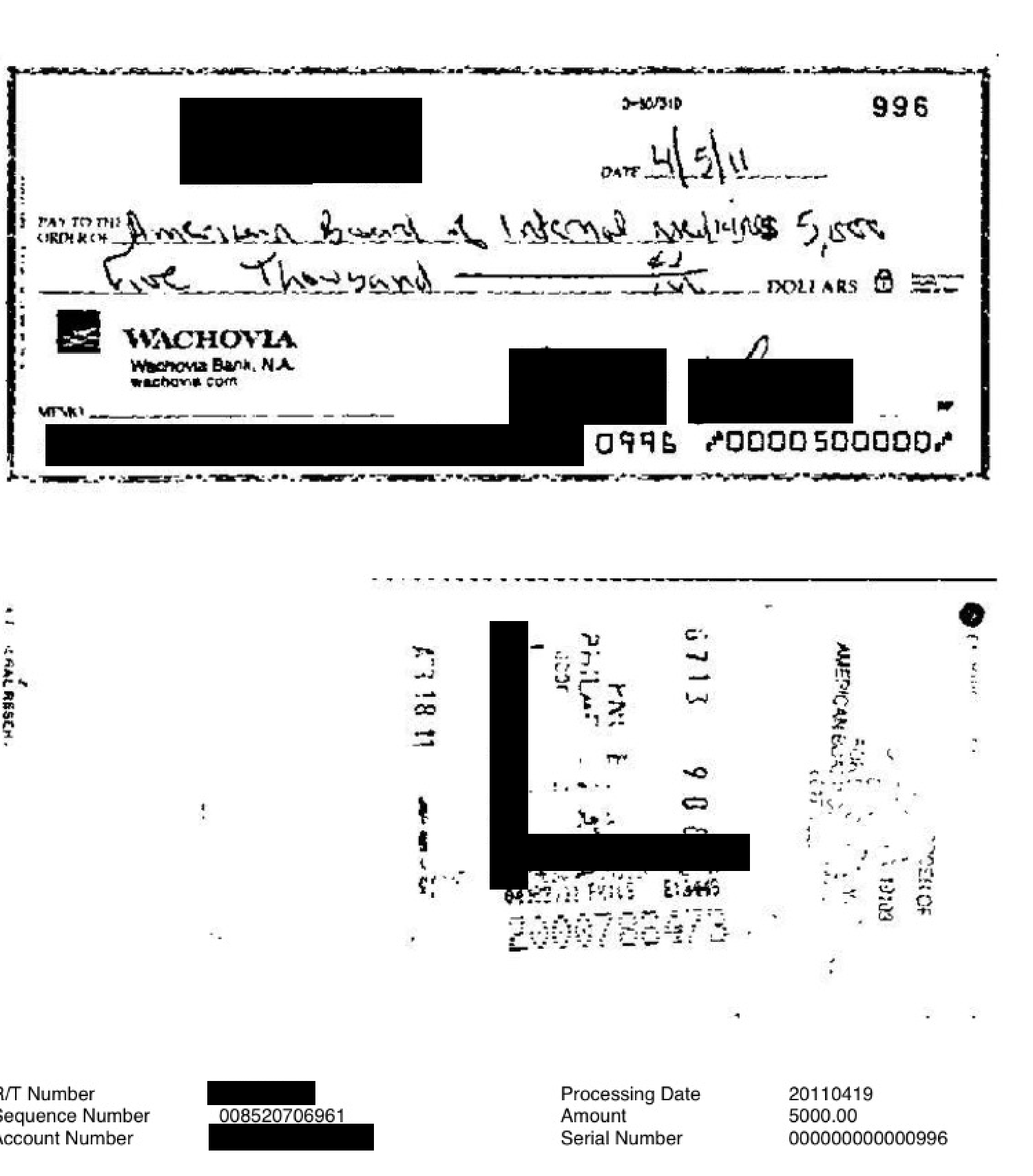
ABIM’s Strongman Tactics
As a result of strongman tactics by the American Board of Internal Medicine (ABIM) in its Arora Board Review investigation, “139 vulnerable physicians (and thousands more who received ‘letters of concern’) had their entire careers threatened…, [resulting in] untold…anxiety, legal fees, and public humiliation before proper due process could occur.” In many cases, physicians were forced to pay hefty fines to reinstate their board certification—so ABIM officials “could maintain their monopoly, power, and lavish executive lifestyles,” writes Westby Fisher, M.D. (https://tinyurl.com/yahufcd6).
“How, where, when, and why [can] unaccountable physician certifying bodies retaliate against or sue physicians by intruding upon their personal property and civil liberties on the basis of an unproven promise of assuring ‘patient safety and physician quality’…?” asks Dr. Fisher. He quotes Michel Foucault, who addresses the relationship between power and knowledge, and how they are used as a form of social control: “Discipline works more subtly, with an exquisite care even, in order to produce obedient people.”
“To limit a physicians’ ability to think critically and… autonomously…creates dangerous consequences for both caregivers and their patients,” Dr. Fisher states.
Labs Bankrupt; Doctors Sued for FCA Damages
Insurers are linking up with bankruptcy trustee attorneys to try to collect False Claims Act damages from thousands of physicians who ordered tests from certain now-bankrupt laboratories. Doctors ordered tests in good faith, but Medicare decided retroactively that it had paid the labs for tests that were “not medically necessary.” Some tests were costing Medicare $1,000 or more per person. Two bankrupt labs allegedly owe Medicare $200 million for overusing tests to detect a rare heart ailment. Some labs were marketing genetic tests as a tool for making pain management safer by pinpointing the proper drugs and dosage for each patient. Private insurers are also taking a closer look at such tests.
Bankruptcy trustees argue that labs paid illegal fees to physicians to induce them to order questionable tests (https://tinyurl.com/y9xomsb9). A judge apparently gave the bankruptcy attorney the ability to demand payment from all physician who had used the company, regardless of guilt, claiming that they had deceived the government.
Correspondence
Delicensed for Failure to Use Computer. In a case that came to national attention, Dr. Anna Konopka, age 84, surrendered her medical license, reportedly for refusing to use a computer and participate in the state’s new online opioid monitoring program. She stated that she only prescribed to a few patients and in small amounts. A New Hampshire judge refused her second request to restore her license, even though she agreed to learn to use a computer and participate in the program. The New Hampshire Union Leader reported that she is under investigation “in a case involving drugs.” Apparently, that stems from a 2016 case in which the police arrested a man who had an opioid prescription from her. When the police tried to return the bottle to her, she suggested putting it in her office mailbox. Reportedly, police then claimed she was using her mailbox to distribute prescription drugs (https://tinyurl.com/y7mpqr6m). This reminds me of the Fitzgibbons case (www.jpands.org/vol18no2/huntoon.pdf), in which police planted a bag of drugs in the doctor’s car.
Like doctors who resign their medical staff privileges when attacked by a sham peer review, doctors who “voluntarily” relinquish their license rarely get it back. They are also surrendering due process rights. Courts usually side with the hospital or board.
Lawrence R. Huntoon, M.D., Ph.D., Lake View, NY
Stealth Rationing. It’s a precarious time for Medicare patients. The Accountable Care Organizations (ACOs) in ACA and alternative Payment Models (APMs) in MACRA are nearly interchangeable. If the ACO/APM protocol does not allow a certain treatment, it probably won’t be available. The electronic health record (EHR) might not allow the order, and it will track clinicians’ compliance. Patients may have no way of knowing that their care is being micromanaged in this way. Without such rationing, Medicare is not sustainable. Officials of both parties believe they can use the law to squeeze doctors to act in certain ways. Patients may want to refrain from using their Medicare “insurance.”
Joseph Guarino, M.D., Reidsville, NC
Self-Pay Patients: When Signing Hospital Admission Form… add the words “Cash Medicare Rates”…and take a photo of the form. When the bills start showing up (there will be many), you must dispute each in writing, within 30 days, with the words, “I feel this billing statement is incorrect.” Demand to be re-invoiced with HCPCS codes and plain English descriptions by line item. It is then possible to determine what the Medicare fee would be in your region (https://tinyurl.com/y89h4gqn), so you will have a basis for negotiation. In circumstances in which pre-negotiation of a price is impossible, many jurisdictions use an “implied contracts approach,” the amount a prudent buyer and seller might have agreed to given adequate time and information (https://tinyurl.com/y9olj36l). Hospitals accept Medicare payment for about 58% of their charges.
Bert McComas, MedicalSelfSufficiency.com
Technocracy. The medical industry used to be medical professionals using technology; it has become a technology industry that uses medical professionals. Each year, the technological behemoth grows larger, and the micro-management of physicians becomes more acute. Technocracy leads to scientific dictatorship, the purpose revealed in 1938 in The Technocrat magazine: Technocracy is the science of social engineering, the scientific operation of the entire social mechanism to produce and distribute goods and services to the entire population. This “science” discards personal relationships in favor of herd management, like in the agricultural industry. This is our future if we do nothing to stop it (https://tinyurl.com/y9bvpwz9).
Patrick Wood https://www.technocracy.news
“Value” Pay. The 2015 MACRA (“doc fix”) law allowed CMS to coerce doctors to become profiteering gatekeepers for HMO-ACO cartels. These utilized 2011 Obama regulatory waivers that skirted anti-trust, anti-fee-splitting, and anti-self-referral (Stark) laws. The goal is to kill fee for service and substitute capitated payment. Ironically, half of future Medicare payments will still be FFS to keep track of “productivity” (how many patients can be crowded into a doctor’s schedule). “Value pay” depends on how much of a corporation’s money a doctor “spends” on care—a productivity measure of value only to the cartels.
As F.R. Abrams pointed out (“Patient Advocate or Secret Agent?” JAMA 1986;256:1784-1785), all managed-care organizations on fixed budgets—the NHS, agencies governed by the 1971 Soviet physician’s oath, U.S. commercial HMOs, or Medicare—all “have in common fidelity to society before fidelity to the patient.” Moreover, “deception and failure to inform are violations of the physician’s fiduciary relationship with the patient.”
Robert W. Geist, M.D., North Oaks, MN


{kind=link}
{kind=link}